ABOUT three months ago, I reported on the Covid-19 situation in Malaysia in the midst of our second wave.
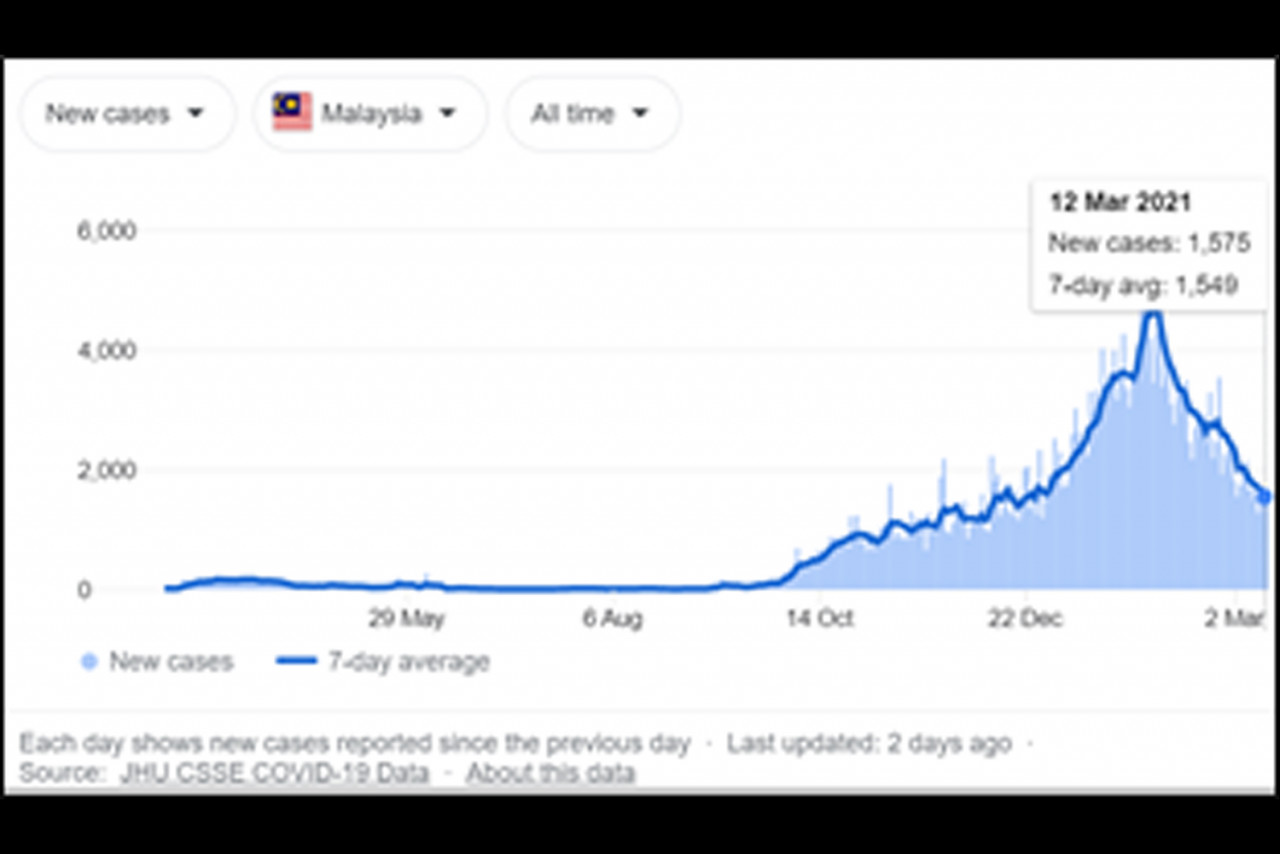
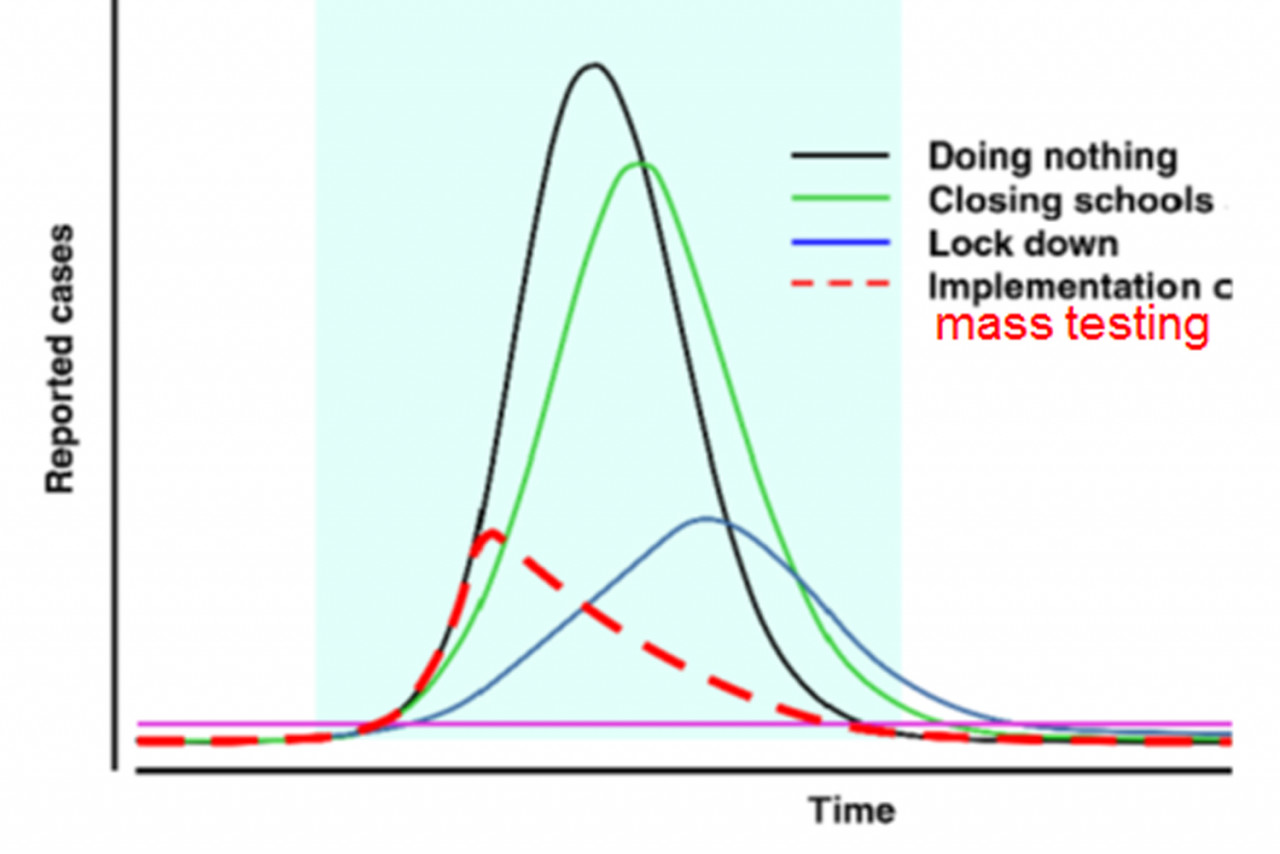
A lockdown was imposed again in January (the second movement control order, or MCO2) – and with the Covid-19 case count coming down in the past weeks (see chart below), the lockdown is just beginning to be lifted.
Many of my fellow Malaysians must be wondering, what’s in store for us? Is this the beginning of the end of our war against Covid-19?
If it’s so predictable, then what’s new?
Given enough time, all lockdowns will work – and so will MCO2. The number of new Covid-19 cases has decreased, to everyone’s relief. Sure, one may argue that the count has decreased in part because we are doing less testing.
But, there can be no dispute that MCO2 works. When one is prepared to lock down a population and restrict them from mingling with each other, whether at work or at play, the virus transmission will certainly decrease – but at the cost of much mental anguish and damage to the economy. It is simply not sustainable, and must be lifted sooner or later.
The second Covid-19 wave in Malaysia is predicated on three factors:
1. Asymptomatic or pre-symptomatic transmissions, which typically account for fewer than 50% of infections;
2. Super-spreading or clustering of transmissions, by which 20% of infected individuals cause about 80% of transmissions; and,
3. The presence of large numbers of migrant workers working and living in crowded conditions.
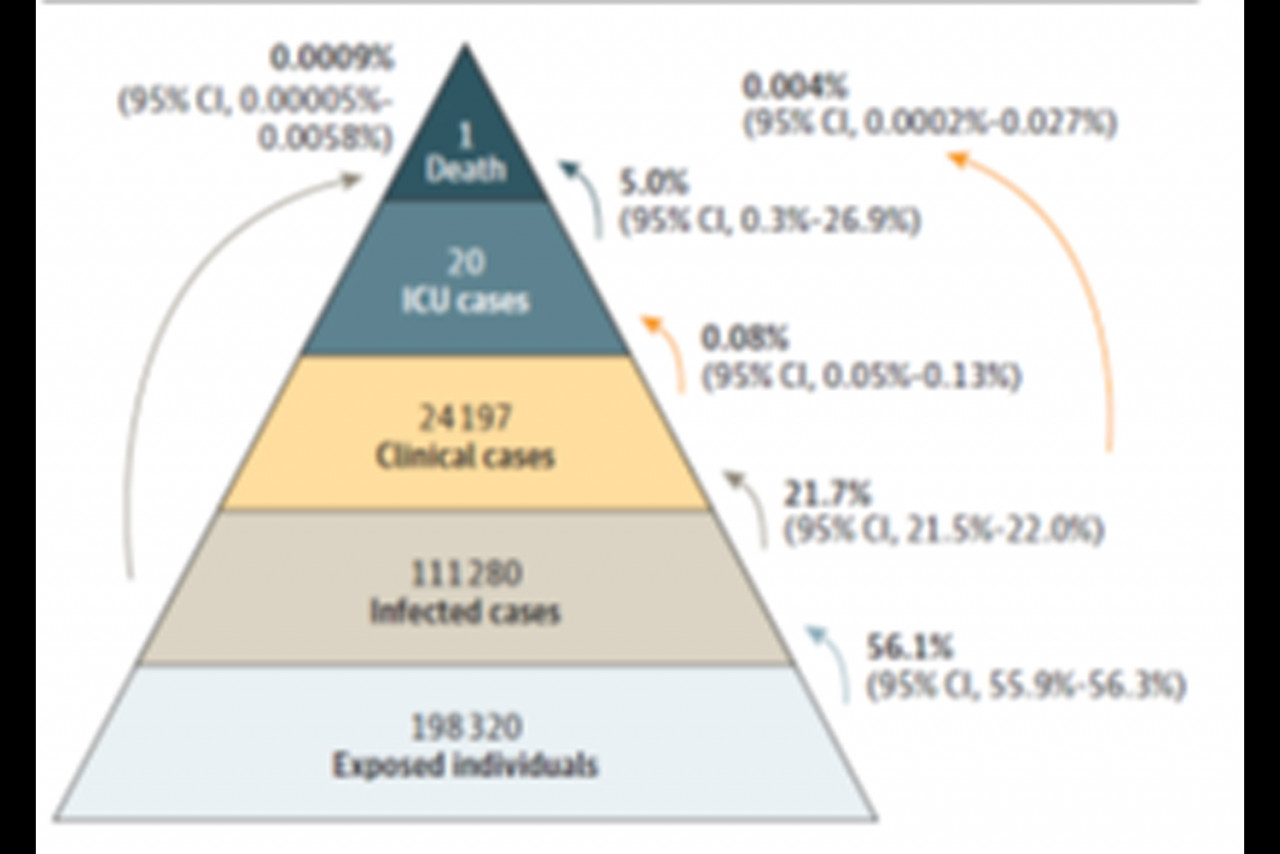
The last factor accounted for the large outbreak in Singapore last year, which was successfully contained. They have subsequently published their data (see figure below), confirming that 56% of workers in dormitories were infected, of whom 22% were symptomatic and only one died (0.001%).
Given that these three factors are still here with us (MCO2 doesn’t eliminate them), let’s not pretend we have seen the worst. What’s next, then? Let’s hope we have used the time so dearly purchased with MCO2 to prepare for the next phase of the war.
To avoid another costly lockdown, we must do two things well: mass vaccination and mass screening.
Mass vaccination
Vaccines work: data from Israel, which was the first country to implement population-wide vaccination, confirms that this is true in the real world, not just in clinical trials.
Vaccines don’t just protect us individually; emerging data suggests that they can stop transmission and prevent asymptomatic infection – thus, herd immunity is achievable, given enough people are vaccinated in a population.
There is no time to waste. Malaysia failed to join the ranks of Asia-Pacific countries that have successfully suppressed Covid-19 through public health measures alone. Unlike these countries, we don’t have the luxury of taking our time to roll out the vaccine.
(Interestingly, Singapore – in typical kiasu fashion – has started vaccination since January, despite being relatively Covid-19-free.)
Our government now has a second chance to prove its mettle to the rakyat – by making sure that all who want to be immunised will receive their shots soon (the anti-vaxxers and vaccine-hesitants can wait till 2022 or later.)
Covid-19 will return as MCO2 winds down; we must act urgently like the UK, the US, Israel, India, Indonesia – countries like us that were unable to suppress Covid-19. They have all rolled out the vaccine, and their performance sets a benchmark for us (see table below).
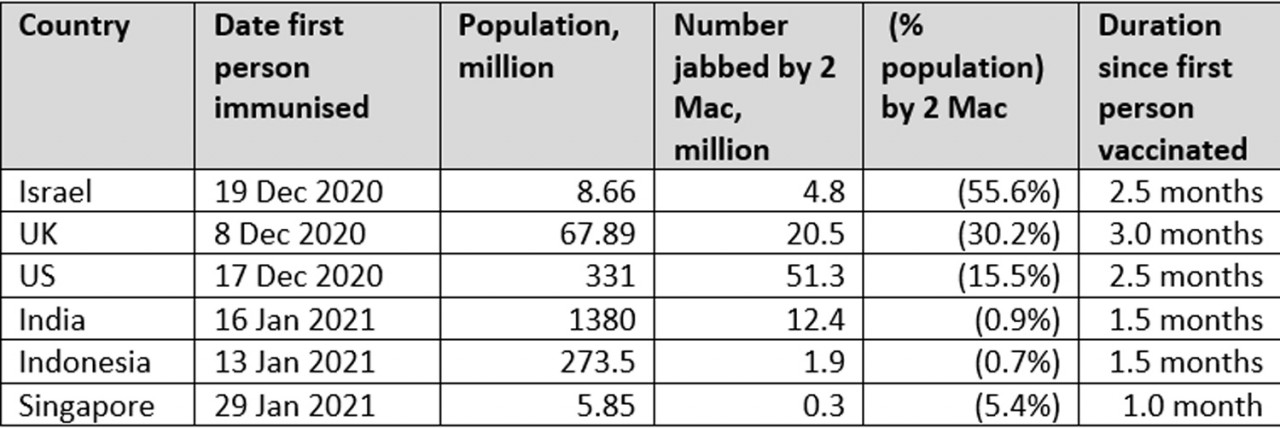
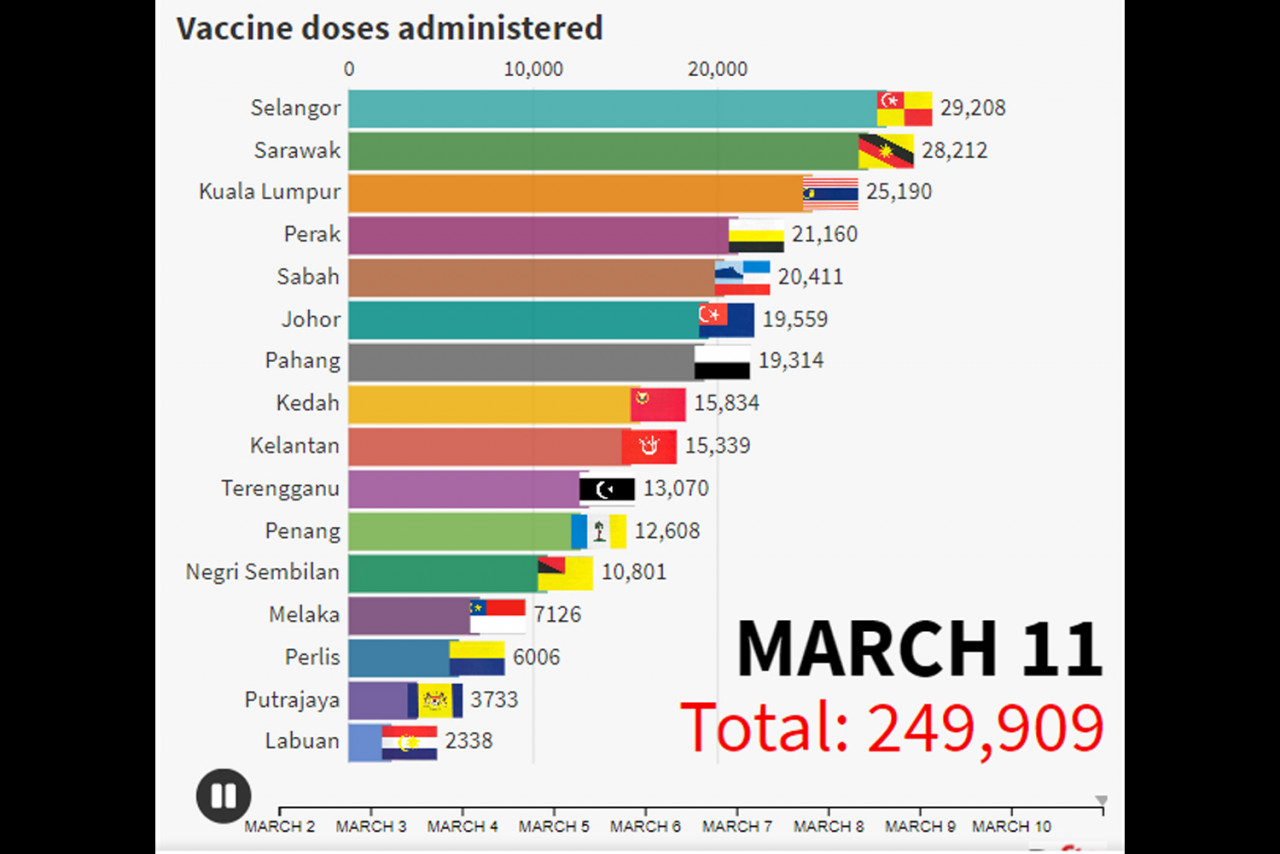
Our prime minister was the first person to be jabbed in Malaysia on February 24 – and as of March 11, about 250,000 frontliners had received their first dose (see chart below). Our government has set itself a target to jab 26 million people (80% of the population) by the end of 2021.
This is a reasonable and achievable target, although it is by no means the fastest schedule in the world (the US did about 20 million in a month, while the UK did seven million in a month) – but let’s not raise the bar and expectations too high.
To meet this target, our government will have to ramp up the vaccination rate quickly, to the tune of 2.7 million people vaccinated per month till year-end. The private healthcare sector should be roped in to assist in these massive efforts – and they are eager to do their part.
Non-conventional delivery channels – such as pharmacies, and on-site vaccination at factories, colleges, etc – should be considered, too. No less critical is community engagement and messaging to get all Malaysians behind these efforts. All must do their part in this war against the virus, the worst crisis we are facing as a nation since World War II.
Mass screening
Covid-19 will return as MCO2 is lifted; businesses are reopening, schools have resumed (my daughter returned to in-person classes two weeks ago), and even social life will start to pick up. Humans are just naturally social; it is not just in our memes (culture), but in our genes as well (yes, there really is such a thing as genes for sociality).
All places where large numbers of people must unavoidably congregate repeatedly and often for a prolonged duration – factories, offices, workers’ dorms, old folks’ homes, schools, college dorms, army barracks, even cruise ships – are potential hotspots for rapid Covid-19 transmission. We know better than most countries after having repeatedly observed many clusters arising first from factories and other workplaces.
We must change our testing strategy, from one focusing on case diagnosis and test-and-trace to a mass screening strategy. All the above-mentioned potential hotspots should implement this.
The idea behind mass screening is simple: detect the infection early, thereby preventing the person from spreading the virus to others. We are already doing this. Everywhere you go, you will have your temperature checked.
This is symptom screening, which unfortunately doesn’t work – because, as shown by the data from Singapore, only 22% of infected workers there had symptoms.
Mass testing works, and it works fast. Indeed, some factories, or even offices, are already doing this. Unfortunately, most employers can only do this biweekly – or worse, monthly, which really is completely useless, but understandable as current PCR or even RTK antigen testing on nose swabs is technically demanding, and hence, costly. It is also uncomfortable and hazardous (swabbing causes sneezing, which discharges potentially infectious droplets). Also, PCR testing has a long turnaround time, which compromises the efficacy of screening.
Like vaccines, advances in medical technology have come to the rescue. Low-cost, technically undemanding rapid tests that can be self-administered (much like home urine pregnancy tests) have become available.
New tests based on new (LAMP, Hybrid capture, CRISPR, etc) or not-so-new (spectroscopy) technologies, which can be conveniently performed on saliva, breath or saline mouthwashes, are emerging, too. High-frequency mass screening is now technically possible and affordable.
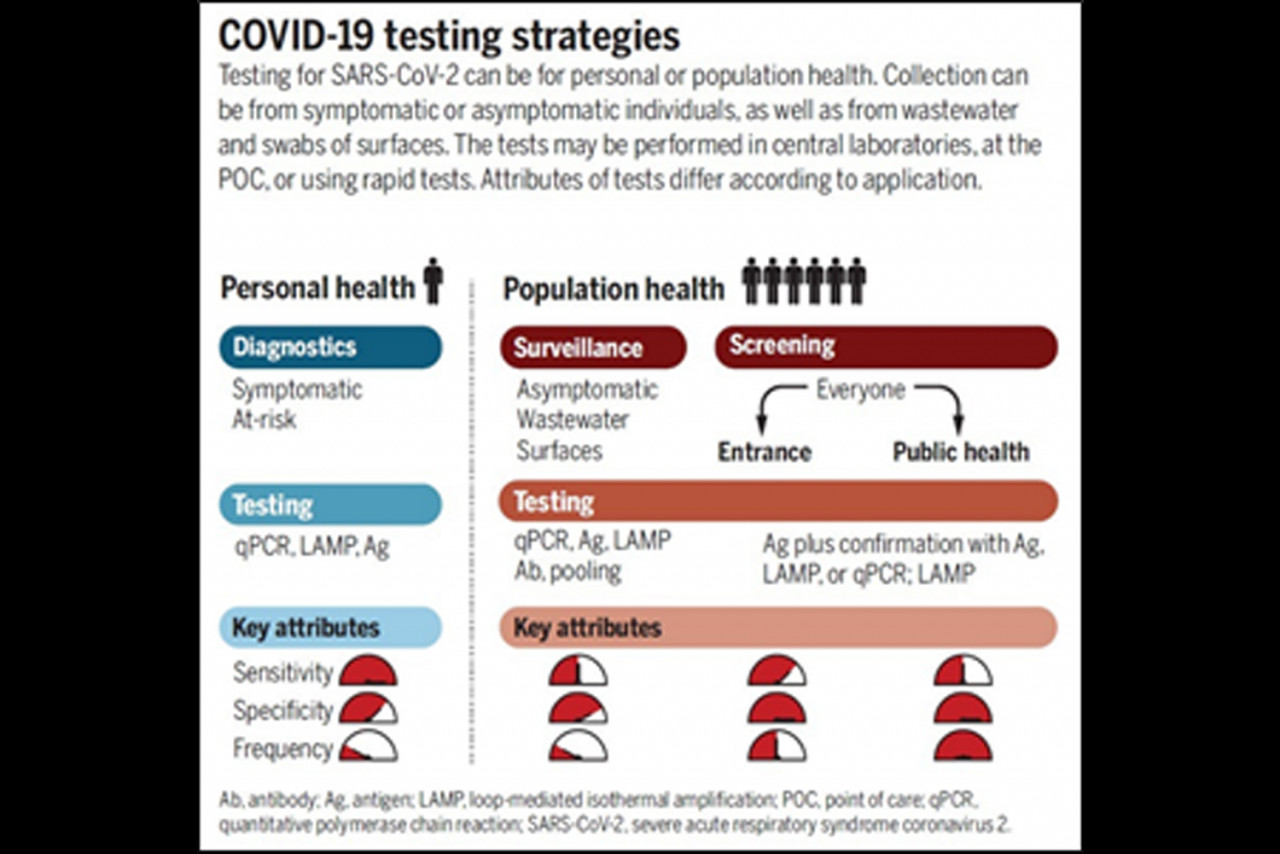
It is important to bear in mind that for the purposes of mass screening (as opposed to the diagnosis of individual patients), test accuracy (measured by test sensitivity or the percentage of false negatives) is much less important than test frequency and turnaround time.
Diagnostic testing requires very accurate tests (95% sensitivity or higher), but paradoxically, a test with, say, 70% sensitivity, but is performed frequently, is superior for screening purposes. This is because current screening tests based on PCR or RTK Ag are too costly to be conducted frequently.
Even wealthy employers can only afford to do these tests, at most, biweekly – which is insufficient. Low-cost, less-sensitive tests (say RM20 per test at 70% sensitivity) conducted twice a week will beat a 99%-sensitivity tests performed once biweekly (you can figure out the maths; overall sensitivity of twice-weekly testing is 99.19%). – The Vibes, April 3, 2021
Dr Lim Teck Onn is a consultant in clinical research and medical statistician