APART from non-pharmaceutical interventions (lockdowns or other restrictions) and vaccination, prophylaxis (treatment given or action taken to prevent disease or its severity) is another pathway to flatten the curve that to date has been given less attention than it deserves.
Vitamin D (VitD), as one of the central elements of our immune system, an inexpensive and relatively safe side effect profile molecule toxic only in extremely high doses, has captivated scientists’ interest as one potential prophylactic since the onset of the Covid-19 pandemic.
The science behind VitD’s crucial immuno-modulating role is long-established through some excellent reviews. Figure 1 summarises some technicalities important to this discussion.
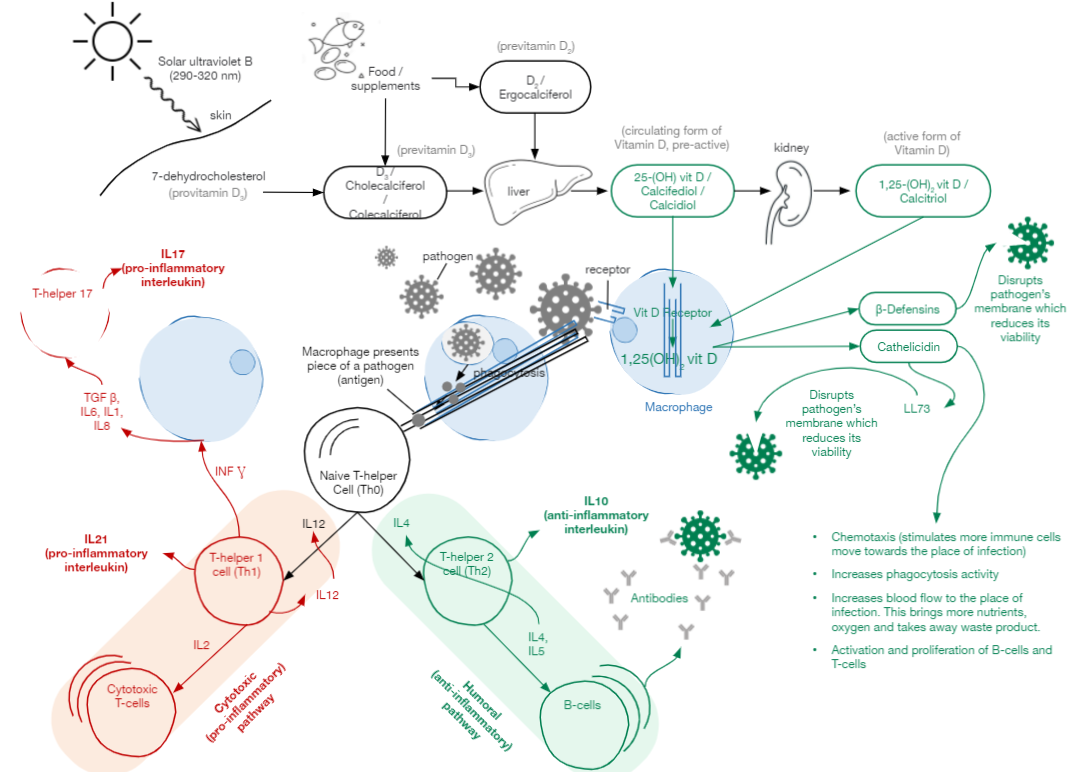
The figure above shows VitD synthesis in our body from its inactive form (D2/D3) to active form through the process of subsequent hydroxylation in our liver and kidney.
VitD helps our innate immune cells to produce beta-defensins and cathelicidins. These peptide nano-soldiers keep the first line of defence (see Figure 1) immediately as a virus enters the body and until the adaptive immune response is activated, which happens in about 7-10 days for the first infection or within 1-2 days in case of reinfection. In other words, even before our B-cells start producing antibodies, beta-defensins and cathelicidins, which can be produced in the right quantity only in VitD sufficiency, can significantly inhibit viral entry into the cells and its replication.
Furthermore, a sufficient level of active VitD inhibits the production of pro-inflammatory cytokines (IL-2, IL-12, IFN-Gamma, IL-6, IL-8, IL-17) while upregulating anti-inflammatory cytokines (IL-4, IL-5, IL-10) (see Figure 1). In other words, VitD down-regulates our immune system response towards the humoral pathway (antibody production), which is less inflammatory and therefore reduces the possibility of the cytokine storm.
VitD has other functions essential in fighting SARS-CoV-2 such as reinforcing physical barrier function in epithelial, intestinal, lung and corneal cells, inducing autophagy of the infected cells, which leads to reduced replication of virus, a mechanism found to be suppressed by SARS-CoV-2. VitD here works similar to ivermectin less its side effects, increasing surfactants that prevent alveolar collapse and many more.
Malaysian health authorities were looking into the VitD and SARS-CoV-2 association at the onset of the pandemic. However, no action was taken due to a lack of sufficient evidence at that time.
Nevertheless, to date, empirical evidence on the close association between SARS-CoV-2 and VitD has multiplied many folds. To get a quick but robust overview of the empirical evidence, it is helpful to look at the most recent systematic meta-analytical studies, which are statistical studies on the large number of empirical studies pooled together (summary statistics in Figure 2).
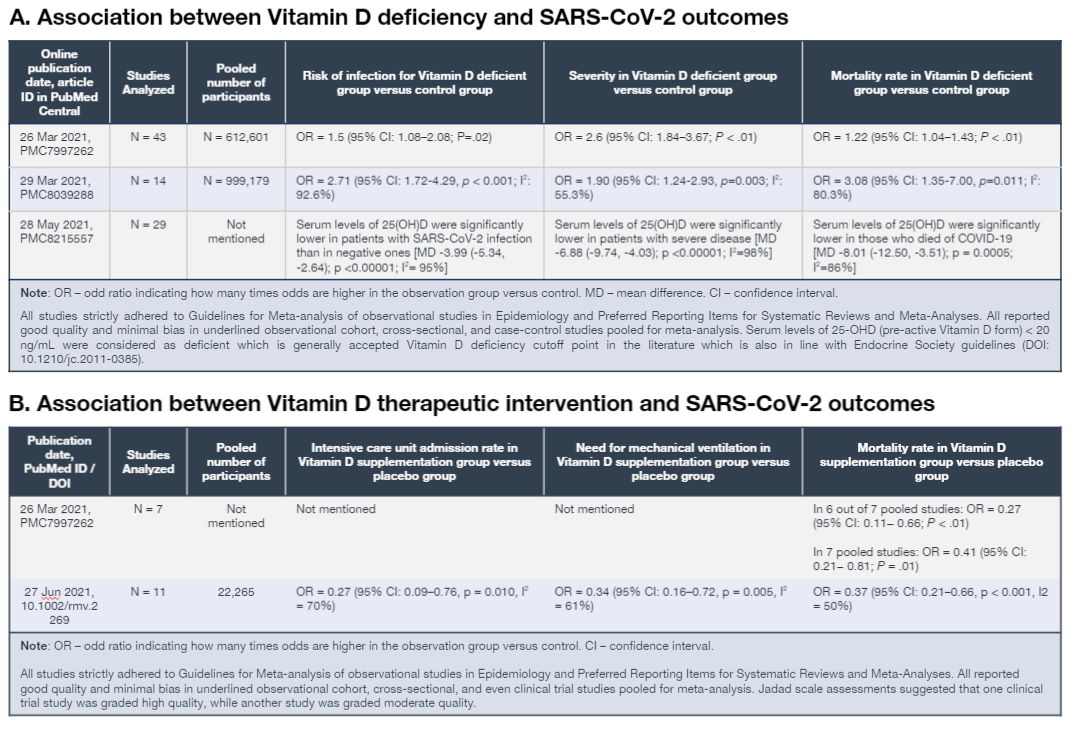
The above systematic reviews of numerous studies (Figure 2a) now convincingly suggest that VitD deficiency defined as 25-OH D < 20 ng/mL is significantly associated with the risk of Covid-19 infection, the severity of its outcomes and mortality.
Although, like some authors rightfully pointed out, association does not imply causation, several clinical trials on VitD supplementation as a therapeutic intervention in SARS-CoV-2 management shed some light on the causal direction.
Two most recent meta-analytic studies (Figure 2b) looked into the existing observational, cross-sectional and even randomised clinical trials for VitD supplementation to SARS-CoV-2 patients and reported the following. The odds of intensive care unit (ICU) admission, need for mechanical ventilation, and mortality were significantly lower in the VitD intervention group than in the placebo group. In all meta-analysed studies, there was inclusion of hypertension, diabetes and corticosteroid use patients. No side effects or adverse events related to VitD intervention are reported.
The above meta-analytic studies did not include another more recent published clinical trial due to the timing of publication. This randomised clinical trial (although single centre) found that therapeutic improvement in serum VitD levels to 80-100 ng/ml has significantly reduced the inflammatory markers associated with Covid-19 with no side-effects. Among the participants, hypertension and diabetes patients were present as well.
The discussion of modes and doses used in any of the above-mentioned clinical trials is intentionally left outside of this article. They are the purview of healthcare specialists and should not be motivation to self-treatment by the general public.
Overall, the convincing empirical results congruent with the well-established theory on VitD are there, but let’s take correct conclusions and corrective measures.
First of all, VitD sufficiency is not a silver bullet against SARS-CoV-2 severity, unlike vaccines. However, VitD deficiency should be recognised at least as a valid and important risk factor for SARS-CoV-2 infection and its severity.
Second, given the accumulated empirical evidence, VitD supplementation intervention in deficiency cases now sounds like a compelling additional strategy to flatten the curve. It is important to note that many studies indicated the importance of early VitD intervention, at least immediately upon admission to the hospital as starting supplementation upon ICU admission could be too late.
Therefore, healthcare authorities could consider making serum VitD deficiency screening standard operating procedure upon a positive RT-PCR test. Early VitD supplementation, in the form of oral vitamin D3 or calcifediol, can be considered for cases with VitD deficiency (25-OH D < 20 ng/mL) and even its insufficiency (25-OH D < 30 ng/mL), which are generally accepted thresholds in the medical literature. This proactive strategy may result in lower hospital admission and subsequent progression of severity while reliving our overwhelmed healthcare system.
Third, this is not in any measure a call for self-treatment! VitD can be toxic in extremely large doses or even in only relatively large doses taken for a prolonged period. Furthermore, unsupervised VitD intake can be risky for people with cardiovascular issues, hypertension, and some other underlying health conditions because the primary function of VitD in our body is to maintain calcium and phosphate levels.
Therefore, unsupervised VitD intake may lead to calcification and other complications. VitD supplementation would also require intake of other essential minerals such as calcium, magnesium, vitamin K2 and others. Therefore, qualified medical assessment, advice and supervision on the mode of intake, correct dosage and duration is the absolute requirement.
Last but not least is the long-term takeaway. The airborne nature of SARS-CoV-2 has taught us that ignoring the state and standards of our ventilation and filtration systems nationwide is a ticking bomb.
Now this virus is drawing our attention to the long-standing problem of VitD deficiency prevalence on the national scale, which to date seems to not have been given the proper attention and intervention. The fact that pandemic management has pushed more people towards the poverty line should ring an even louder alarm, as VitD deficiency is well known to be prevalent in low-income families.
SARS-CoV-2 made our lives miserable in many ways. However, would we be able to appreciate the valuable lessons it taught us? Remember that 99% of the time, crisis management theory talks about the value of being proactive! – The Vibes, July 22, 2021
Rais Hussin and Margarita Peredaryenko are part of the research team at EMIR Research, an independent think tank focused on strategic policy recommendations based on rigorous research