THE pandemic has been ongoing for more than a year now. The light at the end of the tunnel can now be seen. However, this light seems a little too far away for us to feel relieved. I would like to remain hopeful, judging from the overwhelming and positive response to the recent vaccination roll-out in Malaysia.
For vaccinated individuals, there are recommendations on the dos and don’ts. Fully vaccinated individuals (two weeks post-second dose for a two-dose vaccine regimen) are still recommended to wear a mask and practise physical distancing in situations where they are at risk of being exposed to the virus. After all, the pandemic is ongoing, and some regions are having the worst time dealing with the plague right now.
Then, a question struck me: “Why is there a two-week waiting period after the second dose, and why does that matter?” I kept thinking about it. It makes immunological sense to me, but I think there is room for explanation to help the public understand what is happening inside our body in response to the vaccination. Thus, this explainer aims to elucidate the process of generating vaccine-induced immunity and how such immunity is measured.
Before we jump forward, let’s touch base with some facts.
3 facts on Covid-19 vaccination
First, most Covid-19 vaccines protect against severe disease that would otherwise require hospitalisation. Virtually all vaccine clinical trials are designed to count how many people become infected either in the vaccine or placebo group, and how severe the infection is.
As it currently stands, there is limited but encouraging evidence that some vaccines can offer protection against asymptomatic infection, and are also potentially effective at blocking transmission. These two immunity parameters are important; asymptomatic infection accounts for a substantial proportion of SARS-CoV-2 infection (Johansson et al, January 2021), and being able to block transmission means that vaccines are the key to halt the spread. The first parameter is being investigated, while the second requires a different kind of vaccine clinical trial: a human challenge study, i.e. exposing fully vaccinated individuals with the live virus in a very controlled manner (Kirby, October 2020). This is not a totally new concept, and has been done before with the Influenza A virus (Treanor & Wright, 2003).
However, parts of the SARS-CoV-2 biology are still shrouded in mystery, hence the medical and research communities are being told to exercise extreme caution regarding planning for a SARS-CoV-2 human challenge study, along with the ethical consideration of performing such a study.
Second, post-vaccination side effects are something we need to be aware of. Before Covid-19 vaccines made it to the spotlight, vaccine side effects were not as widely discussed. As an anecdotal evidence, I do not recall my annual flu shot causing more than a really sore muscle. The MMR immunisation that I took prior to departing for my study abroad also did not elicit strong side effects, if any. After my second dose of the Covid-19 mRNA vaccine, however, I remember that I had to take a day off because of fatigue, joint pain, chills and muscle soreness. Despite the intensity of the side effects (which some people do not experience at all), they usually do not last longer than a day. In fact, side effects are a good thing. It serves as a proxy measure that the vaccination is working.
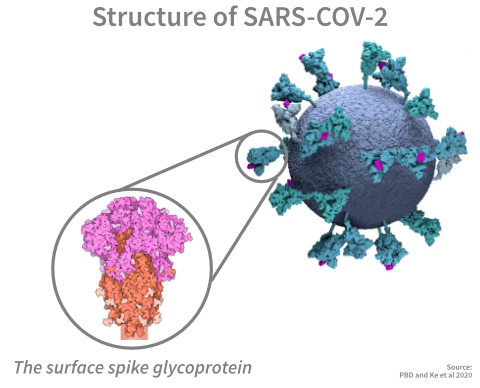
The primary active ingredient in vaccines is certain antigens (usually proteins) derived from the target pathogen. In the SARS-CoV-2 vaccine, the primary active ingredient is the surface spike glycoprotein, or simply, the “spike”. Antigens are commonly inflammatory in nature; they are something our body is not used to seeing, hence, our body would initiate programmes to decisively deal with them. These programmes include raising the body temperature and causing swelling at the injection site to encourage other immune cells to infiltrate that area in order to defend the body from them (Hervé et al, September 2019). However, the spike protein alone is harmless and would not cause any pathology.
Third, immunity from Covid-19 vaccination is estimated to be durable. I have seen discussion on the internet on the waning of antibody levels against SARS-CoV-2. Well, that is to be expected. Antibody, which is a tiny globular protein akin to a molecular handcuff to disarm microscopic threats, does have a shelf-life. It is detectable in the blood for months, and sometimes, years (Wajnberg et al, December 2020). The ebbing of it does not indicate a decline in immunity; it simply means our body decides there is no need to continuously produce it in large quantities.
What is more important is the presence of the T memory and B memory cells. These cells are tasked with generating antibodies under specific conditions, such as re-exposure to the pathogen. Under normal conditions, they are just chilling in your blood doing virtually nothing, akin to living a sedentary life, but not quite a couch potato. Think of the antibody and these memory cells like you are meal-prepping your lunch; the food (antibody) is going to get eaten, but you (memory cells) can always make it. Well, as long as you remember how to make it.
Just a quick note, by the way. It is the B cell that produces antibodies, but it does so effectively with the help of the T cell.
Decades worth of research in infectious disease have shown that these T and B memory cells can last a lifetime once they are generated through infection or vaccination, and our current situation with SARS-CoV-2 has not betrayed this expectation (Baumgarth et al, September 2020). However, there is an exception to the rule: the emergence of SARS-CoV-2 virus variants (a process known as antigenic drift), with some of these variants known to escape immunity. This is not totally new, either, based on what we already know from more than half a century of work with the Influenza A virus and recent work on a common-cold human seasonal coronavirus (Eguia et al, April 2021).
Maybe in a separate discussion, I will go over what we know and what we do not know regarding SARS-CoV-2 and its potential to evade immunity through evolutionary drift during its circulation in the human population.
Measuring protection
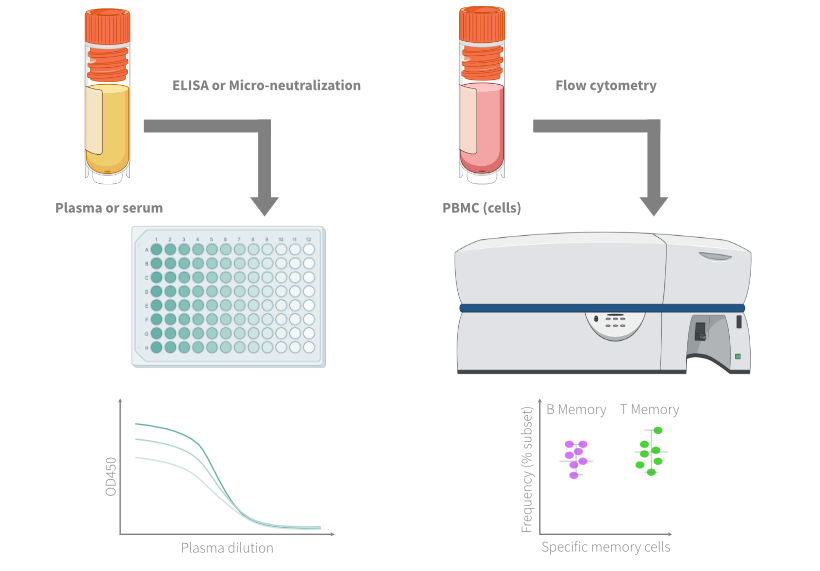
The process to measure protection includes an extensive characterisation of the antibodies circulating in our blood. Additionally, the frequency of specific memory cells can be measured through a variety of lab procedures. Typically, the process to characterise antibody levels is less expensive and requires tooling that is not as sophisticated compared with measuring the frequency of specific memory cells. In this section, we will go over both aspects of measuring antibody levels and the frequency of memory cells, and what information they can provide us.
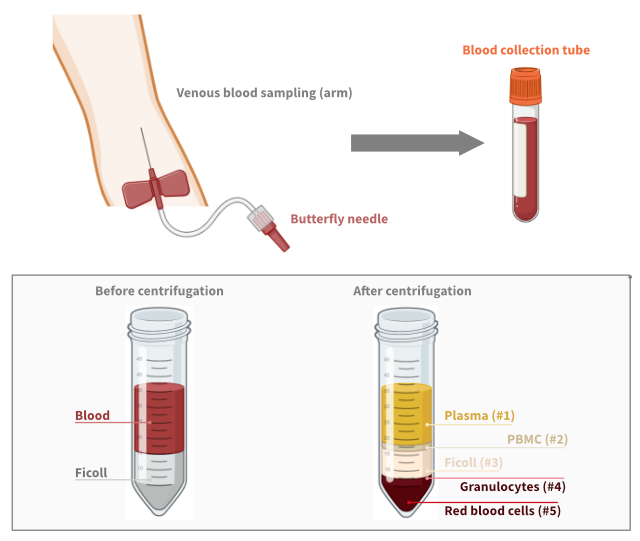
To measure either of them, we first need to draw blood by venous blood sampling. The intended measurements (to measure either antibody levels or the frequency of specific memory cells) dictate the volume to be drawn. The volume needed is usually small, around 20ml to 40ml, which is less than 10% of a hot grande caramel macchiato (470ml). In contrast, we usually donate 400ml (about 8% of the average adult blood volume) during a regular blood donation.
Afterwards, the blood is spun down at high speed (around 2,000rpm) for roughly half an hour. The high centrifugation speed, along with the use of a certain reagent, causes the blood to fractionate into five phases. For characterisation of antibody levels, the plasma (Phase 1) is used. For memory cells, PBMC (Phase 2) is used.
Now, we have the plasma and peripheral blood mononuclear cells (PBMC, containing our immune memory cells). The next step is measuring the immune parameters of interest. We can start by looking at the antibody levels, as this would be the easiest and generally more accessible. For this part, researchers usually break down the measurements into two broad categories: 1) the total levels of a specific antibody, usually measured in concentration (microgramme per millilitre of blood, in μg/ml unit), and 2) the levels of functional antibody, typically measured in plasma dilution (e.g. 1:640 plasma dilution, i.e. the least amount of diluted plasma needed to deactivate a live virus). The former is cheaper and faster to measure, while the latter is time-consuming, but more informative on the degree of protection.
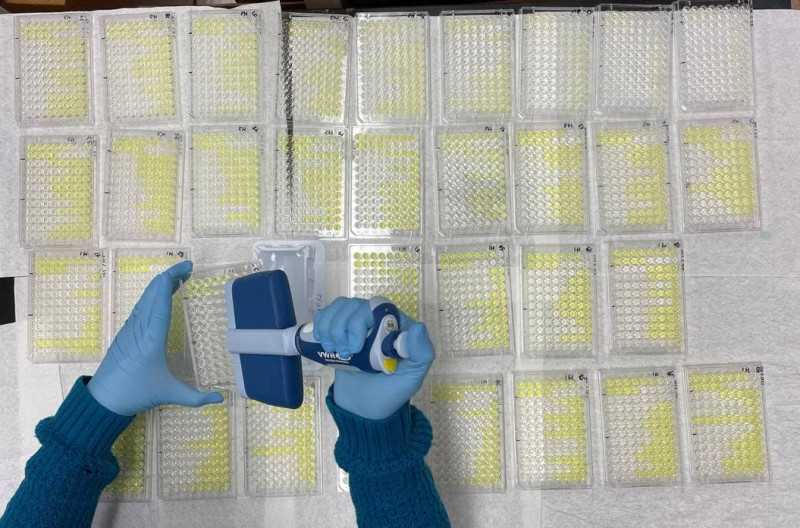
For your additional information, the first method involves a common laboratory procedure known as Elisa (enzyme-linked immunosorbent assay), while the second is commonly known as micro-neutralisation.
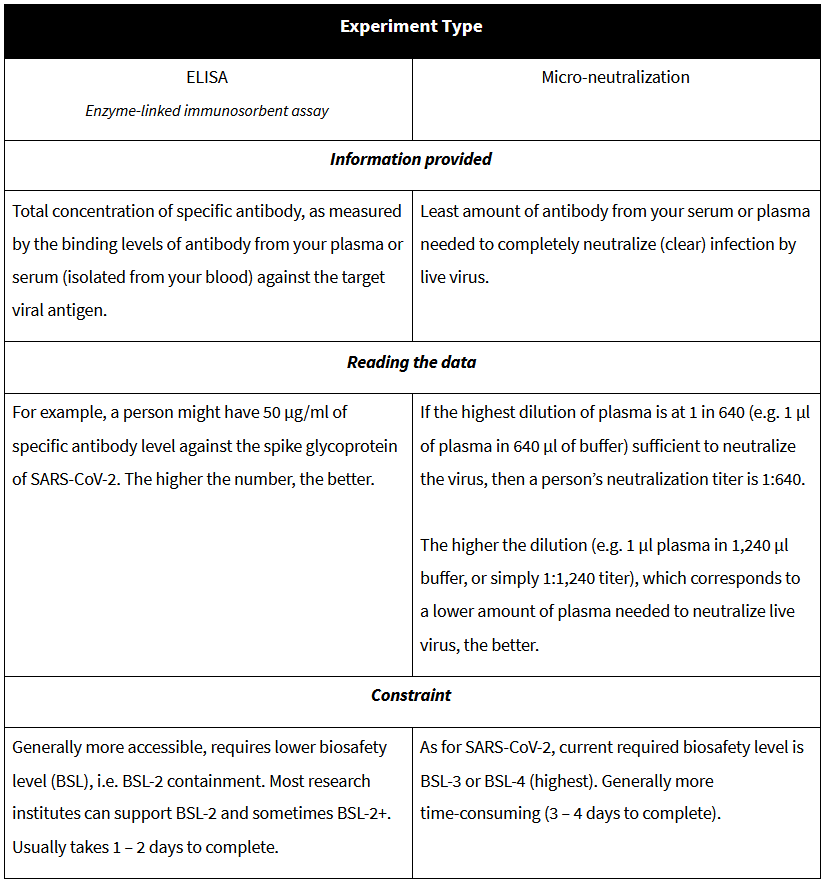
Briefly, the procedure involves the following steps: serially diluting the plasma sample, incubating the plasma sample either in antigen-coated plates (Elisa) or with a live virus (micro-neutralisation), and then measuring the total amount of bound antibodies to antigen (Elisa) or proportion of uninfected cells (micro-neutralisation).
For measuring the frequency of specific immune memory cells, either T memory or B memory cells, the laboratory procedure is much more intricate and requires specialised instruments. The preferred method nowadays is called “flow cytometry”, done by using a class of (very expensive) instrument called “flow cytometer”. In a grossly oversimplified protocol description, the isolated PBMC are stained with multiple fluorescent reporter molecules to denote what kind of cells they are (i.e. T cells are very, very different from B cells), and then, the stained cells are passed through a flow cytometer. Each cell will go through a series of laser beams inside a flow cytometer, which causes the reporter molecules to emit a distinctive fluorescent spectra.
In an equally grossly oversimplified analogy, flow cytometry is like assigning a constellation of celestial bodies (i.e. horoscope) to a person in an attempt to explain their behaviour and personality. If a person is level-headed, then they must be a Gemini, for example. If a person is a boomer trying to be relevant beyond their era, they must be the dead black dwarf star that does not shine anymore, but wants everyone to gravitate to them. The bottom line is, flow cytometry is a laboratory approach to classify cells, and later, enumerate their frequency.
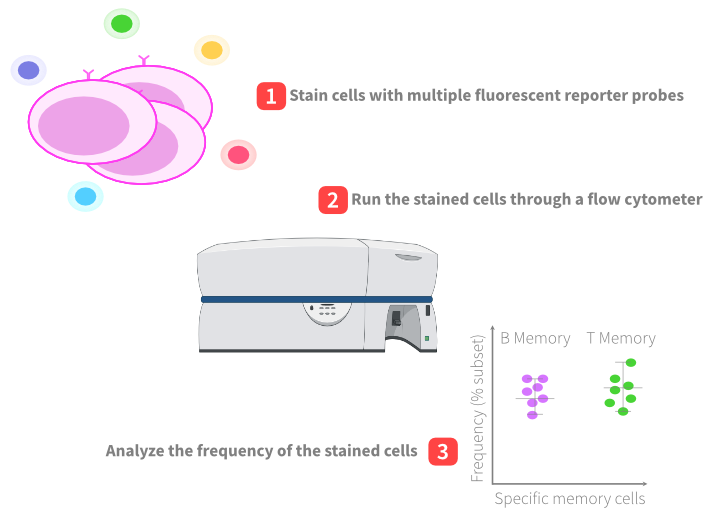
The flow cytometer user would then quantify the emission of fluorescent spectra, and in the end, they would be able to calculate the frequency of specific cells of interest. The readout from flow cytometry is usually expressed as some proportion of numbers, and these numbers usually refer to antigen-specific memory cells as a percentage of the total subset of immune cells. For example, you just measured a total of a million B cells, and of those cells, roughly 4,000 are memory B cells that can recognise the coronavirus spike protein. This translates into 0.4% of specific memory B cell frequency that can recognise the virus.
If you think 0.4% is a low number, bear in mind that there could be hundreds of thousands of them circulating in the body. I would say 0.1% is a pretty good number already, and so, 0.4% after Covid-19 vaccination is a bargain.
Generating protection
Now that we have a basic idea of how we can measure protection, we can start talking about interpreting the data. Specifically, we will now focus on why we need two weeks post-second dose to reap the full benefits of vaccination. Notice that I did not mention all the costs involved in collecting data through the experiments I explained in the prior section, but I bet you could do a pretty extensive analysis on hundreds or thousands of individuals with a RM70 million allocation that would otherwise go to a very well thought-out and modern Covid-19 data integration dashboard system that is somehow... not very well thought-out and modern as purported, on top of being a confusing mess that we are forced to “enjoy” in the aftermath of its premature roll-out.
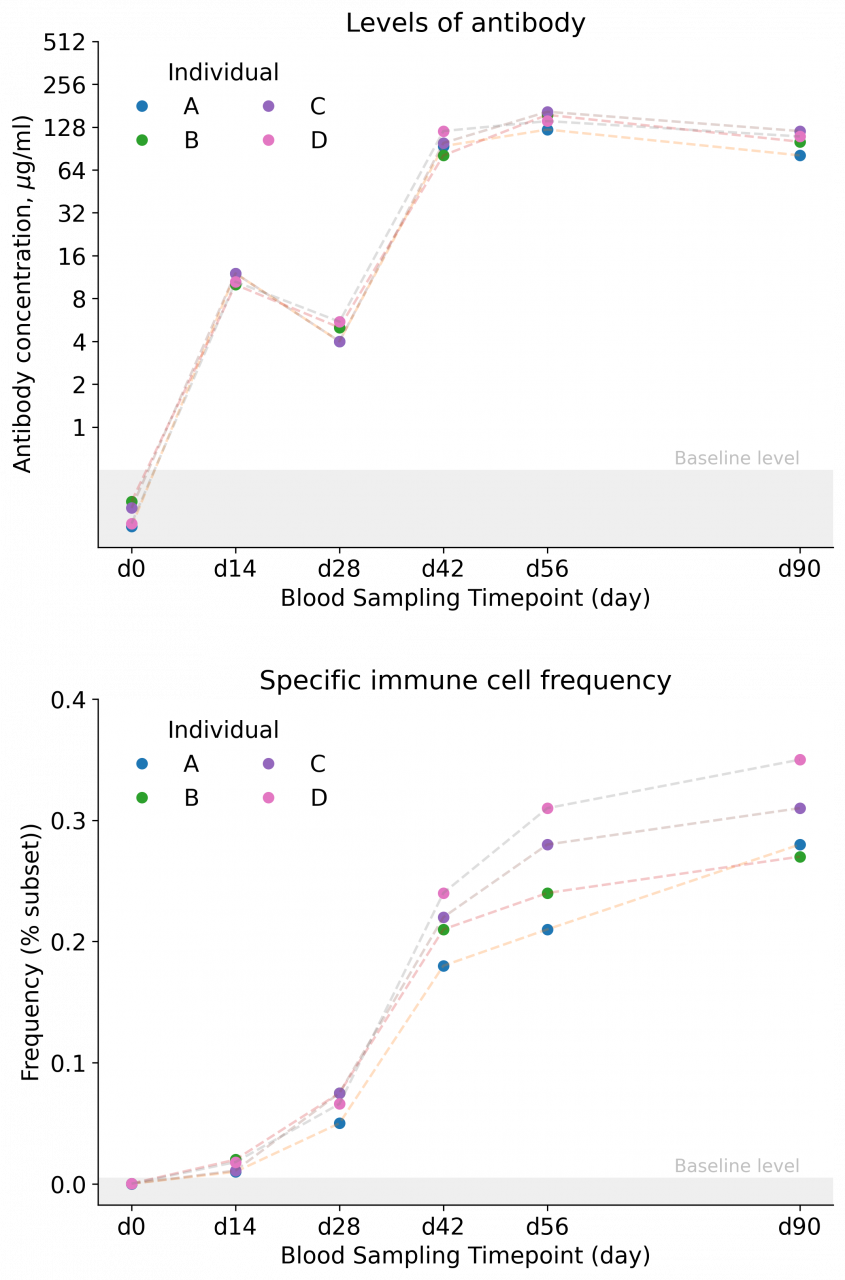
But first, we need to figure out the sampling time points. Having performed analysis on individuals vaccinated for seasonal influenza in the past and for Covid-19 recently, I would be interested to look at the following time points: day 0 before vaccination, days 12 to 14 after the first dose, right before the second dose, days 12 to 14 after the second dose, day 28 after the second dose, and three to six months after the second dose.
This translates into six sampling time points per individual, and would simply be one of the most extensive blood collection schedules. Depending on the intended analysis, usually, the size of the study cohort would be around 20 to 50 individuals. Just quick maths here; 50 individuals multiplied by six sampling time points, and then, multiplied by four tubes per sampling, would total 1,200 tubes of blood. And possibly, many, many hours of lab work, and buckets of sweat and sighs of a criminally underpaid laboratory technician workforce in Malaysia, on top of the constant pandemic fatigue that drains their soul dry. Please, pay your science workforce, and pay them well.
Assuming we have a complete collection of samples, we would expect to see the following trend, on average, across the whole cohort: day 0 would provide basically no signal due to virtually non-existent levels of antibody, then a small and limited increase in the levels of antibody and memory cells on day 14 after the first dose, which would be strongly boosted on day 14 post-second dose, and would remain stable until day 28 post-second dose. As for the levels of antibody, the expectation is that they would gradually decline within three to six months, although likely to remain detectable, while the frequency of immune memory cells would remain stable, even if you look at it a year later.
The question now is: why?
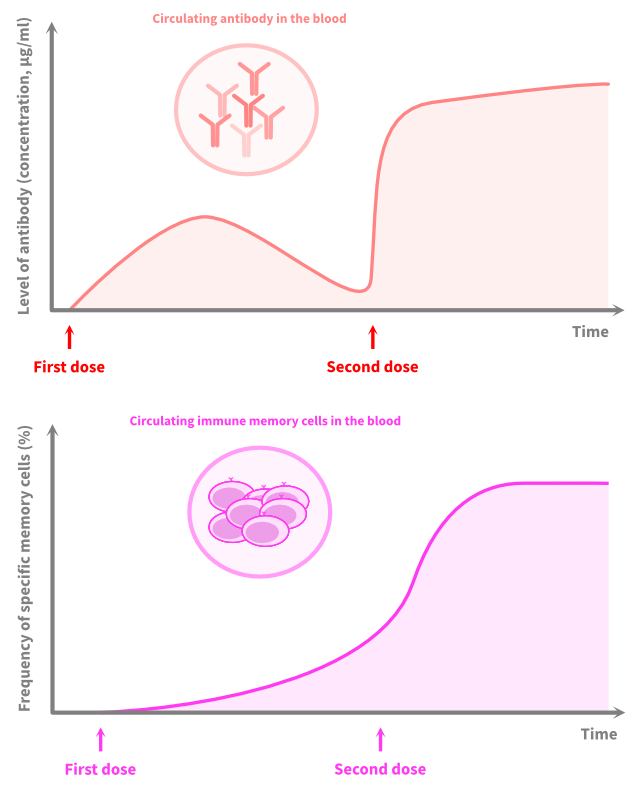
The scientific explanation for this observation can be found in any immunology textbook, in the chapter on “adaptive immune response”, and very likely, you are going to bump into this chart:
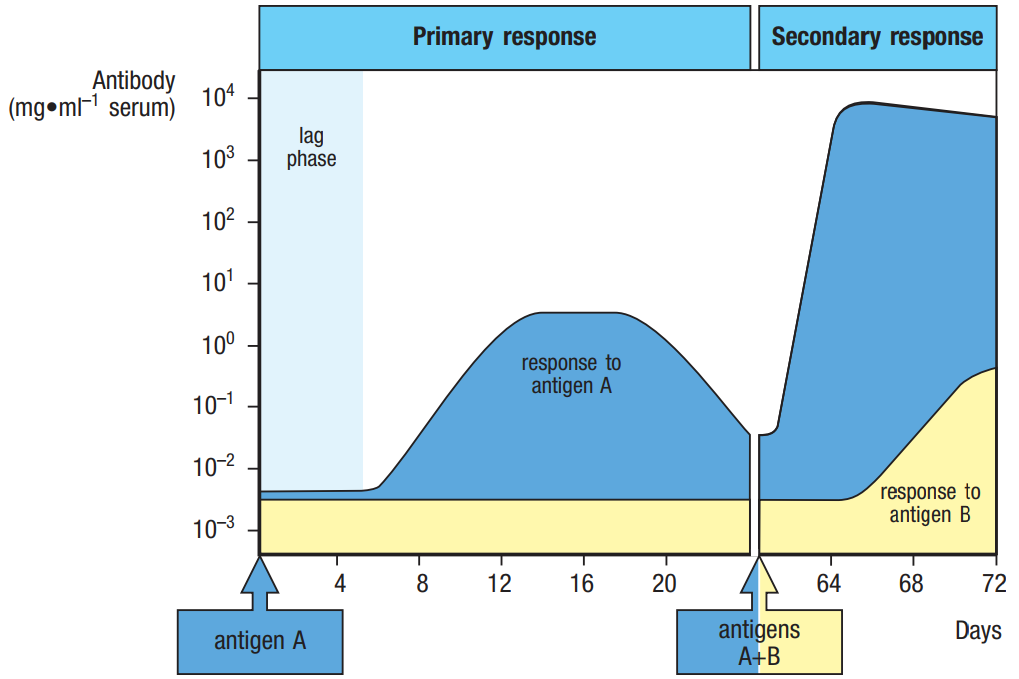
The adaptive immune response is divided into two phases: the primary response (known as naive response) and secondary response (known as memory response). These two phases have very different profiles, both on the kinetics (speed) and magnitude (strength) of the response, and serve as the immunological basis for a two-dose vaccine regimen for offering a strong and lasting immunity.
Unless we are discussing the pre-existing cross-reactive immune response, which is another set of complicated immunological phenomena entirely, it is widely assumed that the levels of antibody on day 0 prior to receiving the vaccine would be virtually zero. With Elisa and/or the micro-neutralisation technique, you would observe a signal that is close to zero, similarly with flow cytometry. On day 14 after the first dose, there would be a small bump. Your body just engaged in a primary response to the vaccination and has been working hard to produce antibodies to the vaccine’s antigen, and at the same time, generating specific immune T and B memory cells.
The kinetics and magnitude of this primary response are slow and limited. If we are asking, “Do we have immunity after the first dose”, the answer would be, “Yes, we do”. However, if the question is, “Is it enough?”, I would answer, “Maybe, I need a bit more”. It is likely that the levels would go down by the time just before the second dose. Again, these are the characteristics of a primary response. It is not well sustained.
Just after receiving the second dose, our immune system engages in a secondary response to the vaccination. This time around, we are activating the T and B memory cells to do the work. As a result, it takes way less time (i.e. faster kinetics) to produce a bucketload of antibodies at a much higher level (i.e. larger magnitude). On day 14 post-second dose, the antibody levels and the frequency of the immune cells would increase several times over.
Can infection happen even after the first dose? The answer is “yes”, it is possible. However, the infection would be limited, to the point that you would not even know it happened because the antibodies in your blood would disarm the virus quickly. Even if the antibody levels are not high, the memory cells would be quick enough to kick-start antibody production, resulting in rapid viral clearance. In other words, your Covid-19 test (e.g. qPCR test) would return positive for the presence of the virus after your second dose, but you would not get sick, and perhaps, be unlikely to transmit it to other people.
So, if you bump into newspaper headlines like “OMG we are doomed, still got infected after receiving Covid-19 vaccine”, just note which newspaper that is, and put it on your browser’s blacklist for engaging in fearmongering and encouraging vaccine hesitancy. We need the pandemic to end, unless we secretly enjoy the movement control order. If that is the case, please seek help. I, for one, am tired and borderline distressed seeing politicians confusing themselves on TV and Twitter. I believe it has been challenging for us not to be angry this Ramadan, and I am annoyed that being a pious Muslim during Ramadan this year has been nothing but near impossible.
Pandemic and the future ahead
The pandemic has been devastating to a lot of societies across the globe. Particularly in our country, with the lack of appropriate responses to it by the federal government, we are further threatened by the prospect of a never-ending plague. However, the recent vaccine roll-out has given us hope that the pandemic will end soon. Based on social media activity during the vaccination sign-up, the signal is clear: the majority of Malaysians would like to be vaccinated. What is left is to educate and share information regarding vaccination to increase confidence in vaccine-induced immunity.
In this explainer, we went through the basic facts to understand the protection offered by vaccination. Then, we went over the basic laboratory protocols to appreciate how immune parameters are measured. Note that these parameters are mostly quantifiable, hence, to provide a simple “yes” or “no” answer is actually challenging. After all, immunity is a gradient, not binary, measure. In other words, understanding the levels of protection is more helpful than to say, “Yes, you have immunity only after two weeks post-second dose”. By knowing the techniques to measure immune parameters, we get to appreciate the nature of immune response, specifically, adaptive immunity, by understanding the two phases of the response: the primary response (after the first dose) and secondary response (post-second dose).
What is left and not covered in this explainer are: 1) how well vaccines are going to protect against variants, as this would be a challenging topic to explain as accurately as possible; 2) the prospect of an evolutionary drifting SARS-CoV-2, much like the Influenza A virus, and its implications for our future; and, 3) in what ways this well-established knowledge in immunology is challenged. I hope this explainer is informative, and if there is any need in the future, we could revisit the lingering questions. – The Vibes, May 15, 2021
Aizan Fahri is a PhD candidate in viral immunology at the David H. Smith Centre for Vaccine Biology and Immunology, University of Rochester Medical Centre, New York